| 规格 | 价格 | 库存 | 数量 |
|---|---|---|---|
| 10 mM * 1 mL in DMSO |
|
||
| 500mg |
|
||
| 1g |
|
||
| 2g |
|
||
| 5g |
|
||
| 10g |
|
||
| 25g |
|
||
| 50g |
|
||
| Other Sizes |
|
| 靶点 |
Endogenous Metabolite
|
|---|---|
| 体外研究 (In Vitro) |
体外活性:黄体酮对乳腺癌细胞的增殖具有双相作用;它刺激第一个细胞周期的生长,然后将细胞阻滞在第二个周期的 G1/S,同时上调细胞周期蛋白依赖性激酶抑制剂 p21。 E1A 的过度表达进一步阻止黄体酮介导的转录,这表明需要 CBP/p300。黄体酮驱动一系列事件,其中管腔细胞可能向基底细胞提供 Wnt4 和 RANKL 信号,基底细胞反过来通过上调其同源受体、转录靶点和细胞周期标记物来做出反应。黄体酮治疗增加皮质突触神经体对 GABA 的敏感性(即降低 EC50)并增加 GABA 刺激 Cl-转运的最大功效(即增加 Emax)。
|
| 体内研究 (In Vivo) |
在小鼠中,黄体酮注射(注射;1 mg;连续每日注射 3 次)可促进子宫内膜血管成熟 [4]。
|
| 细胞实验 |
哺乳动物干细胞(MaSC)位于基底上皮室的一个特殊的小生境中,该小生境受到局部和全身的调节。MaSC在癌症发病中的新作用保证了对MaSC稳态中卵巢激素的研究。在这里,我们发现,在小鼠黄体期的最大孕酮水平期间,MaSC库增加了14倍。富含干细胞的CD49fhi细胞在发情期或外源性黄体酮的情况下扩增,表明黄体酮在推动这种扩增中起着关键作用。在老年小鼠中,CD49fhi细胞在生殖周期停止时表现出停滞。孕酮驱动一系列事件,其中管腔细胞可能向基底细胞提供Wnt4和RANKL信号,基底细胞反过来通过上调其同源受体、转录靶标和细胞周期标记物来做出反应。我们的研究结果揭示了孕酮在生殖周期中激活乳腺干细胞生态位中的成年MaSC的动态作用,其中MaSC是导致癌症的细胞转化事件的假定靶点。[5]
|
| 动物实验 |
Animal/Disease Models: Adult female mice (7-13 wk, 18-28 g)[4]
Doses: 1 mg Route of Administration: Injections; three consecutive daily Experimental Results: Stimulated vessel maturation in the mouse endometrium. |
| 药代性质 (ADME/PK) |
Absorption, Distribution and Excretion
**Oral micronized capsules** Following oral administration of progesterone in the micronized soft-gelatin capsule formulation, peak serum concentration was achieved in the first 3 hours. The absolute bioavailability of micronized progesterone is unknown at this time. In postmenopausal women, serum progesterone concentration increased in a dose-proportional and linear fashion after multiple doses of progesterone capsules, ranging from 100 mg/day to 300 mg/day. **IM administration** After intramuscular (IM) administration of 10 mg of progesterone in oil, the maximum plasma concentrations were achieved in about 8 hours post-injection and plasma concentrations stayed above baseline for approximately 24 hours post-injection. Injections of 10, 25, and 50 mg lead to geometric mean values for maximum plasma concentration (CMAX) of 7, 28, and 50 ng/mL, respectively. Progesterone administered by the intramuscular (IM) route avoids significant first-pass hepatic metabolism. As a result, endometrial tissue concentrations of progesterone achieved with IM administration are higher when compared with oral administration. Despite this, the highest concentrations of progesterone in endometrial tissue are reached with vaginal administration. **Note on oral contraceptive tablet absorption** Serum progestin levels peak about 2 hours after oral administration of progesterone-only contraceptive tablets, followed by rapid distribution and elimination. By 24 hours after drug administration, serum levels remain near the baseline, making efficacy dependent upon strict adherence to the dosing schedule. Large variations in serum progesterone levels occur among individuals. Progestin-only administration leads to lower steady-state serum progestin levels and a shorter elimination half-life than concurrent administration with estrogens. Progesterone metabolites are excreted mainly by the kidneys. Urinary elimination is observed for 95% of patients in the form of glycuroconjugated metabolites, primarily 3 a, 5 ß–pregnanediol (_pregnandiol_). The glucuronide and sulfate conjugates of pregnanediol and pregnanolone are excreted in the urine and bile. Progesterone metabolites, excreted in the bile, may undergo enterohepatic recycling or may be found excreted in the feces. When administered vaginally, progesterone is well absorbed by uterine endometrial tissue, and a small percentage is distributed into the systemic circulation. The amount of progesterone in the systemic circulation appears to be of minimal importance, especially when implantation, pregnancy, and live birth outcomes appear similar for intramuscular and vaginal administration of progesterone. **Apparent clearance** 1367 ± 348 (50mg of progesterone administered by vaginal insert once daily). 106 ± 15 L/h (50mg/mL IM injection once daily). PROMETRIUM Capsules are an oral dosage form of micronized progesterone which is chemically identical to progesterone of ovarian origin. The oral bioavailability of progesterone is increased through micronization. After oral administration of progesterone as a micronized soft-gelatin capsule formulation, maximum serum concentrations were attained within 3 hours. The absolute bioavailability of micronized progesterone is not known. Serum progesterone concentrations appeared linear and dose proportional following multiple dose administration of PROMETRIUM Capsules 100 mg over the dose range 100 mg/day to 300 mg/day in postmenopausal women. Although doses greater than 300 mg/day were not studied in females, serum concentrations from a study in male volunteers appeared linear and dose proportional between 100 mg/day and 400 mg/day. The pharmacokinetic parameters in male volunteers were generally consistent with those seen in postmenopausal women. For more Absorption, Distribution and Excretion (Complete) data for PROGESTERONE (12 total), please visit the HSDB record page. Metabolism / Metabolites Progesterone is mainly metabolized by the liver. After oral administration, the major plasma metabolites found are 20 a hydroxy-Δ4 a-prenolone and 5 a-dihydroprogesterone. Some progesterone metabolites are found excreted in the bile and these metabolites may be deconjugated and subsequently metabolized in the gut by reduction, dehydroxylation, and epimerization. The major plasma and urinary metabolites are comparable to those found during the physiological progesterone secretion of the corpus luteum. Progesterone undergoes both biliary and renal elimination. Following an injection of labeled progesterone, 50-60% of the excretion of progesterone metabolites occurs via the kidney; approximately 10% occurs via the bile and feces, the second major excretory pathway. Progesterone is metabolized primarily by the liver largely to pregnanediols and pregnanolones. Pregnanediols and pregnanolones are conjugated in the liver to glucuronide and sulfate metabolites. Progesterone metabolites which are excreted in the bile may be deconjugated and may be further metabolized in the gut via reduction, dehydroxylation, and epimerization. The major urinary metabolite of oral progesterone is 5beta-pregnan-3alpha, 20alpha-diol glucuronide which is present in plasma in the conjugated form only. Plasma metabolites also include 5beta-pregnan-3alpha-ol-20-one (5beta-pregnanolone) and 5alpha-pregnan-3alpha-ol-20-one (5beta-pregnanolone). The hormone is reduced to pregnanediol in the liver and conjugated with glucuronic acid, and then excreted mainly in urine. For more Metabolism/Metabolites (Complete) data for PROGESTERONE (9 total), please visit the HSDB record page. Progesterone has known human metabolites that include 16beta-hydroxy-progesterone, 17alpha-hydroxy-progesterone, 6beta-hydroxy-progesterone, 2beta-hydroxy-progesterone, and 21-hydroxy-progesterone. Progesterone is metabolized primarily by the liver largely to pregnanediols and pregnanolones. Route of Elimination: The glucuronide and sulfate conjugates of pregnanediol and pregnanolone are excreted in the urine and bile. Progesterone metabolites which are excreted in the bile may undergo enterohepatic recycling or may be excreted in the feces. Progesterone metabolites are excreted mainly by the kidneys. Half Life: 34.8-55.13 hours Biological Half-Life Absorption half-life is approximately 25-50 hours and an elimination half-life of 5-20 minutes (progesterone gel). Progesterone, administered orally, has a short serum half-life (approximately 5 minutes). It is rapidly metabolized to _17-hydroxyprogesterone_ during its first pass through the liver. Due to the sustained release properties of Prochieve, progesterone absorption is prolonged with an absorption half-life of approximately 25-50 hours, and an elimination half-life of 5-20 minutes. Therefore, the pharmacokinetics of Prochieve are rate-limited by absorption rather than by elimination. The elimination half life of progesterone is approximately 5 minutes ... Progesterone has a short plasma half-life of several minutes. |
| 毒性/毒理 (Toxicokinetics/TK) |
Toxicity Summary
Progesterone shares the pharmacological actions of the progestins. Progesterone binds to the progesterone and estrogen receptors. Target cells include the female reproductive tract, the mammary gland, the hypothalamus, and the pituitary. Once bound to the receptor, progestins like Progesterone will slow the frequency of release of gonadotropin releasing hormone (GnRH) from the hypothalamus and blunt the pre-ovulatory LH (luteinizing hormone) surge. In women who have adequate endogenous estrogen, progesterone transforms a proliferative endometrium into a secretory one. Progesterone is essential for the development of decidual tissue and is necessary to increase endometrial receptivity for implantation of an embryo. Once an embryo has been implanted, progesterone acts to maintain the pregnancy. Progesterone also stimulates the growth of mammary alveolar tissue and relaxes uterine smooth muscle. It has little estrogenic and androgenic activity. Interactions Progesterone has been shown to increase cocaine's cardiovascular toxicity in sheep and rats. To determine whether progesterone enhances the lethality of cocaine, 50 non-pregnant female rats were treated with 8 mg/kg/day im progesterone for 3 days, and 45 non-pregnant control rats were given im injections of vehicle (peanut oil, benzoylbenzoate, and phenol). A third group consisted of 21 untreated d16 pregnant rats. On day 3 of injections, rats received one ip injection of cocaine at a dose between 25-75 mg/kg, and were observed for seizures and/or death. Three dose-response curves were constructed using logistic regression analysis. All 51 rats who died did so within 17 minutes, and 49 of these deaths were preceded by sudden seizures. Mean time-to-seizure and time-to-death did not significantly differ among groups. Serum progesterone levels (ng/ml + or - standard error of measurement) were significantly different: 23 + or - 2.3 (control), 102 + or - 9.9 (progesterone treated), and 144 + or - 11.5 (untreated pregnant). Logistic regression dose/fatality curves for the three groups were not significantly different based on the chi-square and likelihood ratio test (p= 0.81). The LD50s in mg/kg ip (95% confidence interval) were (control) 54.8 (49.6-60.5) (progesterone treated) 56.5 (50.3-63.6), and (untreated pregnant) 51.8 (42.2-63.5). Curves of cocaine dose vs isolated seizures plus deaths were not different between control and progesterone treated groups. Though progesterone enhances cocaine's cardiac toxicity, it does not increase the risk of death from acute cocaine exposure in rats. The effects of progesterone treatment on bupivacaine arrhythmogenicity in beating rat heart myocyte cultures and on anesthetized rats were determined. After determining the bupivacaine AD50 (the concentration of bupivacaine that caused 50% of all beating rat heart myocyte cultures to become arrhythmic), the effect of 1 hr progesterone hydrogen chloride exposure on myocyte contractile rhythm was determined. Each concentration of progesterone (6.25, 12.5, 25, and 50 ug/ml) caused a significant and concentration dependent reduction in the AD50 for bupivacaine. Estradiol treatment also increased the arrhythmogenicity of bupivacaine in myocyte cultures, but was only one fourth as potent as progesterone. Neither progesterone nor estradiol effects on bupivacaine arrhythmogenicity were potentiated by epinephrine. Chronic progesterone pretreatment (5 mg/kg/day for 21 days) caused a significant increase in bupivacaine arrhythmogenicity in intact pentobarbital anesthetized rats. There was a significant decrease in the time to onset of arrhythmia as compared with control nonprogesterone treated rats (6.2 + or - 1.3 vs 30.8 + or - 2.5 min, mean + or - standard error). The results of this study indicate that progesterone can potentiate bupivacaine arrhythmogenicity both in vivo and in vitro. Potentiation of bupivacain arrhythmia in myocyte cultures suggests that this effect is at least partly mediated at the myocyte level. 10 mg progesterone injected sc twice weekly into 52 rabbits exposed to vaginal strings containing 3-methylcholanthrene did not affect incidence of vaginal tumors occurring within 20 months, incidences being 5/23 in controls compared with 4/30 in treated animals. Decreased efficacy of some progestins, ... has been suggested to be caused by enhanced metabolism of the progestins by these drugs /hepatic enzyme inducing medications, such as: carbamazepine, phenobarbital, phenytoin, rifabutin, rifampin/. /Progestins/ For more Interactions (Complete) data for PROGESTERONE (6 total), please visit the HSDB record page. |
| 参考文献 |
[1]. Schindler AE, et al. Classification and pharmacology of progestins. Maturitas. 2003 Dec 10;46 Suppl 1:S7-S16.
[2]. Zava DT, et al. Estrogen and progestin bioactivity of foods, herbs, and spices. Proc Soc Exp Biol Med. 1998 Mar;217(3):369-78. [3]. Komesaroff PA, et al. Effects of wild yam extract on menopausal symptoms, lipids and sex hormones in healthy menopausal women. Climacteric. 2001 Jun;4(2):144-50. [4]. Girling JE, et al. Progesterone, but not estrogen, stimulates vessel maturation in the mouse endometrium. Endocrinology. 2007 Nov;148(11):5433-41. Epub 2007 Aug 9. [5]. Progesterone induces adult mammary stem cell expansion. Nature. 2010 Jun 10;465(7299):803-7. |
| 其他信息 |
Therapeutic Uses
Progestins Prochieve 4% is indicated for the treatment of secondary amenorrhea. Prochieve 8% is indicated for use in women who have failed to respond to treatment with Prochieve 4%. /Included in US product label/ Prochieve 8% is indicated for progesterone supplementation or replacement as part of an Assisted Reproductive Technology ("ART") treatment for infertile women with progesterone deficiency. /Included in US product label/ Progesterone is used orally or intravaginally for the management of secondary amenorrhea. For more Therapeutic Uses (Complete) data for PROGESTERONE (9 total), please visit the HSDB record page. Drug Warnings /BOXED WARNING/ WARNING: CARDIOVASCULAR DISORDERS, BREAST CANCER and PROBABLE DEMENTIA FOR ESTROGEN PLUS PROGESTIN THERAPY. Cardiovascular Disorders and Probable Dementia: Estrogens plus progestin therapy should not be used for the prevention of cardiovascular disease or dementia. The Women's Health Initiative (WHI) estrogen plus progestin substudy reported increased risks of deep vein thrombosis, pulmonary embolism, stroke and myocardial infarction in postmenopausal women (50 to 79 years of age) during 5.6 years of treatment with daily oral conjugated estrogens (CE) (0.625 mg) combined with medroxyprogesterone acetate (MPA) (2.5 mg), relative to placebo. The WHI Memory Study (WHIMS) estrogen plus progestin ancillary study of the WHI reported an increased risk of developing probable dementia in postmenopausal women 65 years of age or older during 4 years of treatment with daily CE (0.625 mg) combined with MPA (2.5 mg), relative to placebo. It is unknown whether this finding applies to younger postmenopausal women. Breast Cancer: The WHI estrogen plus progestin substudy also demonstrated an increased risk of invasive breast cancer. In the absence of comparable data, these risks should be assumed to be similar for other doses of CE and MPA, and other combinations and dosage forms of estrogens and progestins. Progestins with estrogens should be prescribed at the lowest effective doses and for the shortest duration consistent with treatment goals and risks for the individual woman. Other doses of oral conjugated estrogens with medroxyprogesterone and other combinations and dosage forms of estrogens and progestins were not studied in the WHI clinical trials. In the absence of comparable data and product-specific studies, the relevance of the WHI findings to other products has not been established. Therefore, the risks should be assumed to be similar for all estrogen and progestin products. Because of these risks, estrogens with or without progestins should be prescribed at the lowest effective doses and for the shortest duration consistent with treatment goals and risks for the individual woman. Adverse effects reported in patients receiving oral progesterone include dizziness, breast pain, headache, abdominal pain, fatigue, viral infection, abdominal distention, musculoskeletal pain, emotional lability, irritability, and upper respiratory tract infection. Extreme dizziness and/or drowsiness, blurred vision, slurred speech, difficulty walking, loss of consciousness, vertigo, confusion, disorientation, and shortness of breath have been reported in a few women receiving the drug. Hypotension and syncope have occurred rarely in women receiving progesterone capsules. Adverse effects reported in patients receiving progesterone vaginal gel include breast pain/enlargement, somnolence, constipation, nausea, headache, and perineal pain. For more Drug Warnings (Complete) data for PROGESTERONE (19 total), please visit the HSDB record page. Pharmacodynamics Progesterone, depending on concentration and dosage form, and timing of exposure may have several pharmacodynamic effects. These actions, according, to various preparations, are listed below: General effects Progesterone is the main hormone of the corpus luteum and the placenta. It acts on the uterus by changing the proliferative phase to the secretory phase of the endometrium (inner mucous lining of the uterus). This hormone, stimulated by a hormone called _luteinizing hormone_ (LH) is the main hormone during the secretory phase to prepare the corpus luteum and the endometrium for implantation of a fertilized ovum. As the luteal phase concludes, the progesterone hormone sends negative feedback to the anterior pituitary gland in the brain to decrease FSH (follicle stimulating hormone) and LH (luteinizing hormone) levels. This prevents ovulation and maturation of oocytes (immature egg cells). The endometrium then prepares for pregnancy by increasing its vascularity (blood vessels) and stimulating mucous secretion. This process occurs by progesterone stimulating the endometrium to decrease endometrial proliferation, leading to a decreased uterine lining thickness, developing more complex uterine glands, collecting energy in the form of glycogen, and providing more uterine blood vessel surface area suitable for supporting a growing embryo. As opposed to cervical mucous changes observed during the proliferative phase and ovulation, progesterone decreases and thickens the cervical mucus, rendering it less elastic. This change occurs because the fertilization time period has passed, and a specific consistency of mucous amenable to sperm entry is no longer required. **Gelatinized capsules** Progesterone capsules are an oral dosage form of micronized progesterone which, chemically identical to progesterone of ovarian origin. Progesterone capsules have all the properties of endogenous progesterone with induction of a secretory phase endometrium with gestagenic, antiestrogenic, slightly antiandrogenic and anti-aldosterone effects. Progesterone opposes the effects of estrogen on the uterus, and is beneficial in women with unopposed estrogen exposure, which carries an increased risk of malignancy. **Vaginal gel and vaginal insert** The gel preparation mimics the effects of naturally occurring progesterone. In the presence of adequate levels of estrogen, progesterone converts a proliferative endometrium into secretory endometrium. This means that the endometrium changes from a growing and thickening stage into a subsequent preparation stage for pregnancy, which involves further preparatory changes. Progesterone is necessary for the development of decidual tissue (specialized tissue amenable to supporting a possible pregnancy). Progesterone is required to increase endometrial receptivity for the implantation of a fertilized embryo. Once an embryo is implanted, progesterone helps to maintain the pregnancy. **Injection (intramuscular)** Intramuscularly injected progesterone increases serum progesterone and aids in the prevention of endometrial tissue overgrowth due to unopposed estrogen (which leads to abnormal uterine bleeding and sometimes uterine cancer),. In the absence or deficiency of progesterone, the endometrium continually proliferates, eventually outgrowing its limited blood supply, shedding incompletely, and leading to abnormal and/or profuse bleeding as well as malignancy. **Tablets, contraceptive** Progesterone-only contraceptive tablets prevent conception by suppressing ovulation in about half of users, causing a thickening of cervical mucus to inhibit sperm movement, lowering the midcycle LH and FSH hormone peaks, slowing the movement of the ovum through the fallopian tubes, and causing secretory changes in the endometrium as described above. |
| 分子式 |
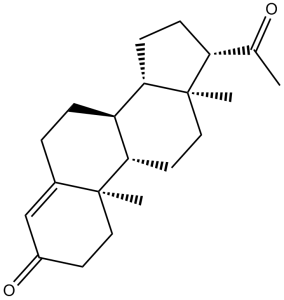
C21H30O2
|
|
|---|---|---|
| 分子量 |
314.46
|
|
| 精确质量 |
314.224
|
|
| 元素分析 |
C, 80.21; H, 9.62; O, 10.18
|
|
| CAS号 |
57-83-0
|
|
| 相关CAS号 |
Progesterone (Standard);57-83-0;Progesterone-d9;15775-74-3;Progesterone-13C5;2687960-32-1;Progesterone-13C3;327048-87-3;Progesterone-13C2;82938-07-6
|
|
| PubChem CID |
5994
|
|
| 外观&性状 |
White to off-white solid powder
|
|
| 密度 |
1.1±0.1 g/cm3
|
|
| 沸点 |
447.2±45.0 °C at 760 mmHg
|
|
| 熔点 |
128-132 °C(lit.)
|
|
| 闪点 |
166.7±25.7 °C
|
|
| 蒸汽压 |
0.0±1.1 mmHg at 25°C
|
|
| 折射率 |
1.542
|
|
| LogP |
4.04
|
|
| tPSA |
34.14
|
|
| 氢键供体(HBD)数目 |
0
|
|
| 氢键受体(HBA)数目 |
2
|
|
| 可旋转键数目(RBC) |
1
|
|
| 重原子数目 |
23
|
|
| 分子复杂度/Complexity |
589
|
|
| 定义原子立体中心数目 |
6
|
|
| SMILES |
O=C(C([H])([H])[H])[C@@]1([H])C([H])([H])C([H])([H])[C@@]2([H])[C@]3([H])C([H])([H])C([H])([H])C4=C([H])C(C([H])([H])C([H])([H])[C@]4(C([H])([H])[H])[C@@]3([H])C([H])([H])C([H])([H])[C@@]21C([H])([H])[H])=O
|
|
| InChi Key |
RJKFOVLPORLFTN-UHFFFAOYSA-N
|
|
| InChi Code |
InChI=1S/C21H30O2/c1-13(22)17-6-7-18-16-5-4-14-12-15(23)8-10-20(14,2)19(16)9-11-21(17,18)3/h12,16-19H,4-11H2,1-3H3
|
|
| 化学名 |
(8S,9S,10R,13S,14S,17S)-17-acetyl-10,13-dimethyl-1,2,6,7,8,9,11,12,14,15,16,17-dodecahydrocyclopenta[a]phenanthren-3-one
|
|
| 别名 |
|
|
| HS Tariff Code |
2934.99.9001
|
|
| 存储方式 |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
|
| 运输条件 |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| 溶解度 (体外实验) |
|
|||
|---|---|---|---|---|
| 溶解度 (体内实验) |
配方 1 中的溶解度: ≥ 2.08 mg/mL (6.61 mM) (饱和度未知) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (这些助溶剂从左到右依次添加,逐一添加), 澄清溶液。
例如,若需制备1 mL的工作液,可将100 μL 20.8 mg/mL澄清DMSO储备液加入400 μL PEG300中,混匀;然后向上述溶液中加入50 μL Tween-80,混匀;加入450 μL生理盐水定容至1 mL。 *生理盐水的制备:将 0.9 g 氯化钠溶解在 100 mL ddH₂O中,得到澄清溶液。 配方 2 中的溶解度: ≥ 2.08 mg/mL (6.61 mM) (饱和度未知) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (这些助溶剂从左到右依次添加,逐一添加), 澄清溶液。 例如,若需制备1 mL的工作液,可将 100 μL 20.8 mg/mL澄清DMSO储备液加入900 μL 20% SBE-β-CD生理盐水溶液中,混匀。 *20% SBE-β-CD 生理盐水溶液的制备(4°C,1 周):将 2 g SBE-β-CD 溶解于 10 mL 生理盐水中,得到澄清溶液。 View More
配方 3 中的溶解度: ≥ 2.08 mg/mL (6.61 mM) (饱和度未知) in 10% DMSO + 90% Corn Oil (这些助溶剂从左到右依次添加,逐一添加), 澄清溶液。 配方 4 中的溶解度: 20 mg/mL (63.60 mM) in 50% PEG300 50% Saline (这些助溶剂从左到右依次添加,逐一添加), 悬浊液; 超声助溶。 *生理盐水的制备:将 0.9 g 氯化钠溶解在 100 mL ddH₂O中,得到澄清溶液。 1、请先配制澄清的储备液(如:用DMSO配置50 或 100 mg/mL母液(储备液)); 2、取适量母液,按从左到右的顺序依次添加助溶剂,澄清后再加入下一助溶剂。以 下列配方为例说明 (注意此配方只用于说明,并不一定代表此产品 的实际溶解配方): 10% DMSO → 40% PEG300 → 5% Tween-80 → 45% ddH2O (或 saline); 假设最终工作液的体积为 1 mL, 浓度为5 mg/mL: 取 100 μL 50 mg/mL 的澄清 DMSO 储备液加到 400 μL PEG300 中,混合均匀/澄清;向上述体系中加入50 μL Tween-80,混合均匀/澄清;然后继续加入450 μL ddH2O (或 saline)定容至 1 mL; 3、溶剂前显示的百分比是指该溶剂在最终溶液/工作液中的体积所占比例; 4、 如产品在配制过程中出现沉淀/析出,可通过加热(≤50℃)或超声的方式助溶; 5、为保证最佳实验结果,工作液请现配现用! 6、如不确定怎么将母液配置成体内动物实验的工作液,请查看说明书或联系我们; 7、 以上所有助溶剂都可在 Invivochem.cn网站购买。 |
| 制备储备液 | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.1801 mL | 15.9003 mL | 31.8005 mL | |
| 5 mM | 0.6360 mL | 3.1801 mL | 6.3601 mL | |
| 10 mM | 0.3180 mL | 1.5900 mL | 3.1801 mL |
1、根据实验需要选择合适的溶剂配制储备液 (母液):对于大多数产品,InvivoChem推荐用DMSO配置母液 (比如:5、10、20mM或者10、20、50 mg/mL浓度),个别水溶性高的产品可直接溶于水。产品在DMSO 、水或其他溶剂中的具体溶解度详见上”溶解度 (体外)”部分;
2、如果您找不到您想要的溶解度信息,或者很难将产品溶解在溶液中,请联系我们;
3、建议使用下列计算器进行相关计算(摩尔浓度计算器、稀释计算器、分子量计算器、重组计算器等);
4、母液配好之后,将其分装到常规用量,并储存在-20°C或-80°C,尽量减少反复冻融循环。
计算结果:
工作液浓度: mg/mL;
DMSO母液配制方法: mg 药物溶于 μL DMSO溶液(母液浓度 mg/mL)。如该浓度超过该批次药物DMSO溶解度,请首先与我们联系。
体内配方配制方法:取 μL DMSO母液,加入 μL PEG300,混匀澄清后加入μL Tween 80,混匀澄清后加入 μL ddH2O,混匀澄清。
(1) 请确保溶液澄清之后,再加入下一种溶剂 (助溶剂) 。可利用涡旋、超声或水浴加热等方法助溶;
(2) 一定要按顺序加入溶剂 (助溶剂) 。
Comparing the Pharmacokinetics of a Progesterone Ring Versus a Progesterone Vaginal Insert
CTID: NCT06668896
Phase: Phase 1 Status: Not yet recruiting
Date: 2024-11-01
 ET receptor antagonist 1
ET receptor antagonist 1
 ERα degrader 6
ERα degrader 6
 hFSH-β-(33-53) (TFA)
hFSH-β-(33-53) (TFA)
 Bisphenol AF-d4 (BPAF-d4; 4,4'-(Perfluoropropane-2,2-diyl)diphenol-d4)
Bisphenol AF-d4 (BPAF-d4; 4,4'-(Perfluoropropane-2,2-diyl)diphenol-d4)
InvivoChem的所有产品仅用于作科学研究,不面向患者销售
Copyright 2020 InvivoChem LLC | All Rights Reserved 粤ICP备20063088号-1






























 COA
COA
