| 规格 | 价格 | 库存 | 数量 |
|---|---|---|---|
| 1mg |
|
||
| 5mg |
|
||
| 10mg |
|
||
| Other Sizes |
|
| 靶点 |
Central complement component C3 (KD = 0.5 nM)
|
|---|---|
| 体外研究 (In Vitro) |
Amyndas Pharmaceuticals临床开发了新一代高选择性和强效的C3抑制剂,称为compstatins Cp40/AMY-101,用于各种补体介导的适应症。这些小型肽C3抑制剂是灵长类/人类特异性的,与之前被评估为ARDS治疗选择的补体抑制剂TP-10等大型生物制剂相比,它们显示出更有利的药理学特征和更大的组织穿透能力[2]。
鉴于基于compstatin-based抑制剂(如AMY-101)的C3阻断可以通过阻断参与SARS-CoV-2诱导的ARDS和血栓性微血管病的所有下游促炎介质的同时产生,提供比抗C5或抗C5a药物更广泛的治疗复盖面,AMY-101作为新冠肺炎感染严重病例中的抗炎剂,可以很好地进行临床评估[2]。 |
| 体内研究 (In Vivo) |
对于患有自然发生的慢性牙周炎的 NHP,AMY-101 可以帮助改善牙周健康 [1]。 AMY-101 可产生持久的抗炎作用 [1]。皮下注射 AMY-101(4 毫克/公斤体重,每 24 小时一次,持续 28 天)可显着且持续地降低 PPD(组织破坏的指标)[1]。在 UUO 诱导的肾纤维化中,AMY-101(Cp40,1 mg/kg,每 12 小时皮下注射一次,每天一次,持续 7 或 14 天)可减少纤维化和炎症细胞浸润 [3]。
局部给药的AMY-101(0.1 mg/部位)不会对健康牙龈造成刺激[1] 为了确定在NHP中施用肽C3抑制剂AMY-101后可能出现的局部牙龈刺激,在五只动物的健康后牙牙龈中注射了治疗剂量的AMY-101(50μL 2mg/mL溶液,相当于0.1mg/部位)30。每只动物共接受四次注射,每象限一次;两次注射使用AMY-101,另外两次注射涉及含有5%葡萄糖的注射用水(WFI)(对照)。在每只动物中,在上颌和下颌象限(共2个部位)注射AMY-101,而在对侧的两个部位注射对照溶液。在第0、7和14天共注射AMY-101和对照溶液三次,然后进行2周的观察期,不再注射。在基线检查时(第0天)和每2-3天拍摄一次口腔照片,以记录注射部位周围的牙龈状况。仔细的日常临床检查显示,在整个观察期间注射AMY-101或对照溶液后没有刺激迹象(图1)。在第-1天和第15天采集血液样本,并进行血液学和生化分析。所有动物的所有测量值均在正常范围内(未显示)。 AMY-101即使每3周服用一次,也能提供保护[1] 我们之前已经证明,每周龈内注射AMY-101可以改善患有自然慢性牙周病的NHP的牙周状况。30不那么频繁但仍然成功的给药将促进AMY-101在人类中的应用。为了探索这种可能性,我们测试了AMY-101在给药频率较低的情况下是否也有效。为此,5只动物每2周服用一次2-mg/mL的AMY-101溶液,另外5只动物则每3周服用一次AMY-101。具体而言,AMY-101被局部注射到上颌骨两侧的前牙和后牙的牙龈中(共17个部位;牙齿之间的腭乳头[15个部位],第三磨牙的远端牙龈[2个部位])。在整个研究过程中,在基线和1、2、4、6、7、8、10和12周进行了临床检查,以确定疾病的进展和AMY-101的潜在有益作用。AMY-101注射前的临床读数作为基线对照。下颌骨未接受治疗,但在整个研究过程中通过临床牙周检查进行监测,以进行比较。该研究包括6周的AMY-101治疗(治疗期),随后6周不进行AMY-101处理(随访期)。 无论给药频率如何,AMY-101都会显著降低测量牙周炎症(GI和探诊出血[BOP])或组织破坏(PPD和CAL)的临床指标(图4和图5)。有趣的是,基线和后续读数之间的差异在6周时或之后达到了统计学意义(即,在AMY-101治疗停止的时间点)。即使在12周时,6周时观察到的许多差异仍然具有统计学意义(BOP、PPD和CAL)(图4B-4D和5B-5D)。在相同的12周间隔内,还监测了未经治疗的颌骨(下颌骨)的上述临床指标。与AMY-101治疗的上颌骨临床状况的改善相比,下颌骨的临床指标在研究过程中与基线值相比没有显示出显著差异(图4和图5)。综上所述,AMY-101可以诱导持久的临床抗炎作用。 全身注射AMY-101可以改善NHPs的牙周状况[1] 鉴于AMY-101也被考虑用于全身性疾病,牙周炎是一种非常普遍的疾病,34我们测试了AMY-101在全身给药时是否有效。AMY-101以4mg/kg体重的浓度通过皮下注射在10只动物中给药,每24小时一次,共28天。为了确定疾病的进展和AMY-101的潜在有益作用,在基线(第0周)和整个研究期间(第1、2、3、4和11周的时间点)进行了临床检查。此外,在基线、4周和11周时对牙龈和骨骼进行了活组织检查。 系统给药AMY-101可显著长期降低PPD,PPD是衡量组织破坏的指标(图6A)。在第4周首次观察到保护作用。令人惊讶的是,即使在第4周后停药,保护作用仍持续至少7周(第11周)而没有下降(图6A)。还观察到评估牙周炎症的BOP有所改善;与基线相比的差异在第2周和第3周达到统计学意义(图6B)。4周时的组织学观察表明,与基线表达相比,AMY-101导致牙槽骨附近结缔组织中促炎和促破骨细胞因子(白细胞介素[IL]-17和核因子κB配体受体激活剂[RANKL])的表达降低,骨保护素(OPG;RANKL的天然抑制剂)的表达升高(图7)。此外,AMY-101处理导致补体切割片段C3d和C5a减少,进一步证实了其抑制补体激活的能力。总之,全身性AMY-101改善了NHPs的牙周状况,在停药后至少7周内保持稳定。 C3缺乏可减轻UUO诱导的肾纤维化中的纤维化和炎性细胞浸润[3] 为了研究C3在UUO发病机制中的作用,我们使用了一种肽C3抑制剂,Compstatin类似物AMY-101/Cp40来阻断C3的激活。Masson染色和α-SMA表达分析表明,注射1mg/kg Cp40的UUO小鼠的间质纤维化程度远低于注射对照肽的小鼠(补充图3A-D)。Western blot分析还表明,注射Cp40的UUO小鼠的α-SMA和PDGFR-β水平降低(补充图3E、F)。除了减轻的肾小管间质纤维化外,与注射肽的小鼠相比,注射Cp40的UUO小鼠的F4/80+巨噬细胞、CD3+T细胞、CD4+T细胞和CD8+T细胞的肾浸润显著减少(图5A-E)。同时,Cp40显著限制了UUO小鼠MCP-1、IL-6、IL-1β和TNF-αmRNA表达的升高(图5F)。这些数据表明,C3介导T细胞和巨噬细胞在梗阻性损伤时浸润肾脏。 阻断C3-C3aR信号通过抑制UUO小鼠中IL-17A的产生来减轻肾纤维化[3] 如图7A所示,与假对照组小鼠相比,UUO小鼠肾脏IL-17A的mRNA水平显著升高。此外,与假对照小鼠血清中的IL-17A水平相比,UUO小鼠血清中IL-17A水平在早期和晚期显著升高(图7B)。与ELISA和mRNA数据一致,FACS结果显示,UUO后梗阻肾脏中8.48%和10.9%的CD4+肾细胞分别表达IL-17A,而假手术小鼠中≤5.3%的CD4+表达IL-17A+,这种作用被AMY-101/Cp40和SB290157强烈抑制(图7C-H)。此外,我们分析了C3阻断UUO小鼠和UUO小鼠肾脏中CD11b+F4/80+IL-17+细胞的比例。结果显示,两组单核细胞中CD11b+F4/80+IL-17+细胞约占1%,用CP40阻断C3后仅略有变化(补充图4A、B)。在14天的UUO小鼠中也证实了类似的结果(补充图4C,D)。因此,我们确定UUO小鼠中IL-17A的主要产生者是T细胞,单侧输尿管结扎后T细胞显著增加。 |
| 细胞实验 |
PBMC分离[3]
患者和正常受试者捐献了5毫升肝素化管中收集的血液。用PBS将血液1:1稀释,并覆盖在淋巴细胞分离培养基上。离心后,收集3ml含有PBMC的界面,用PBS稀释至6ml,然后用冷PBS洗涤两次并计数。收集PBMC进行流式细胞术分析。 CFSE标签[3] 通过将冻干的CFSE溶解在DMSO中新鲜制备CFSE储备溶液(5mM)。从幼年小鼠的脾脏中获得脾细胞,并在37°C下用PBS中5μM的CFSE标记15分钟。通过加入三倍体积的冰冷FBS并在冰上孵育细胞5分钟来淬灭过量的CFSE。然后用PBS洗涤CFSE标记的细胞三次,并在有或没有刺激的情况下培养。 T细胞活化[3] 将预涂有抗CD3和抗CD28抗体的96孔检测板在37°C下孵育4小时。从幼年小鼠的脾脏中获得脾细胞(1×106个细胞/孔),并在含有IL-2(10 ng/mL)、IL-12(10μg/mL)或IL-4(4 ng/mL的培养基中在96孔板中培养3天。 流式细胞术分析[3] 制备单个肾细胞悬浮液,用PMA/离子霉素/高尔基体塞刺激4小时。将细胞与不同的一抗或适当的同种型对照抗体在4°C下孵育30分钟。使用PerCP/Cy5.5结合的抗人CD14抗体;PerCP/Cy5.5联合抗小鼠CD4;APC偶联抗小鼠F4/80;以及PerCP/Cy5.5结合的抗小鼠CD11b。细胞表面染色后,用Cytofix/Cytoperm Soln试剂盒固定和渗透细胞,用Alexa Fluor 488偶联的抗人C3和PE偶联的抗小鼠IL-17A进行细胞内染色。所有流式细胞术分析均使用LSR II流式细胞仪和Flowjo软件进行。 ELISA[3] 为了量化肾脏中的IL-17A水平,根据制造商的说明使用小鼠IL-17A ELISA分析样本。所有测量均进行了两次。 |
| 动物实验 |
动物/疾病模型: 15 只成年雄性食蟹猴(Macaca fascicularis)(7-15 岁;体重 5.0-7.6 kg)[1]。
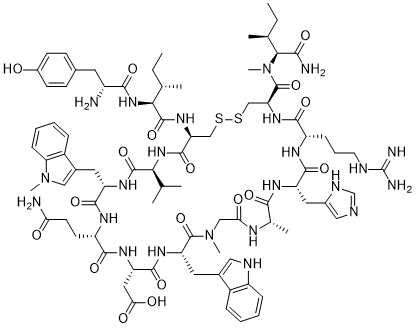
剂量: 0.1 mg/部位;50 μL 浓度为 2 mg/mL 的溶液。 给药途径: 局部注射。(每周 3 次或每周 1 次,持续 6 周,然后进行 6 周的随访,无需治疗。) 实验结果: 对健康牙龈无刺激。 动物/疾病模型: 单侧输尿管梗阻 (UUO) 小鼠和假手术小鼠 [3]。 剂量: 1 mg/kg。 给药途径:每 12 小时皮下注射一次,每日一次,持续 7 或 14 天。 实验结果: 1 mg/kg Cp40 引起的间质纤维化程度显著低于注射该肽的对照小鼠。 C3 抑制剂 AMY-101 [1] 14 残基 compstatin 类似物 AMY-101 [(D)Tyr-Ile-[Cys-Val-Trp(Me)-Gln-Asp-Trp-Sar-Ala-His-Arg-Cys]-mIle-NH2,其中 Sar 为肌氨酸/N-甲基甘氨酸,mIle 为 N-甲基异亮氨酸] 采用固相肽合成方法,如前所述,以二硫键桥联的环状肽形式制备。使用 30G 短针将不同浓度(2–200 mg/mL)的 AMY-101 局部注射到牙龈(50 μL)。或者,对于全身给药,使用配备 28G × 1/2 英寸针头的 1 mL 胰岛素安全注射器进行皮下注射(4 mg/kg 体重)。 临床检查和观察 [1] 进行临床牙周检查,并根据美国牙周病学会制定的人类牙周疾病诊断标准进行诊断。在基线和整个研究期间使用牙周探针进行检查,以监测疾病进展和 AMY-101 治疗的效果。检查项目包括:探诊深度(PPD,测量牙龈缘至牙周袋底部的距离,单位为毫米)、临床附着丧失(CAL,测量釉牙骨质界至牙周袋底部的距离)、牙菌斑指数(GI,根据Löe分级,0-3级)、出血指数(BOP,阳性位点百分比)和菌斑指数(PI,根据Löe分级,0-3级)。PPD、CAL和BOP在每颗牙齿的六个位点进行测量:近颊侧、颊侧中部、远颊侧、近舌侧、舌侧中部和远舌侧。GI和PI在四个位点进行评估(颊侧、舌侧、近中侧和远中侧)。GI和BOP是牙周炎症的指标,而CAL和PPD评估组织破坏程度。PI是牙面生物膜积聚的临床指标。在刺激性研究中,每日对注射部位进行临床观察,以监测炎症迹象或脓肿、发红、瘙痒、血肿、瘀伤、水疱或结节的形成。牙龈炎症程度评估为健康、轻度(颜色轻微变化,无出血)、中度(发红,出血)或重度(明显发红,易自发性出血)。 动物模型[3] 单侧输尿管梗阻(UUO)是一种常用的肾损伤实验模型。对6-8周龄的小鼠进行麻醉,然后在小鼠背部做侧切口。随后,暴露左侧输尿管,并用两根4.0丝线结扎。假手术组小鼠接受相同的手术操作,但不进行输尿管结扎。本治疗实验采用固相肽合成法制备的Compstatin类似物AMY-101/Cp40 (dTyr-Ile-[Cys-Val-Trp(Me)-Gln-Asp-Trp-Sar-His-Arg-Cys]-mIle-NH2;1.7kDa)和购自Sigma-Aldrich公司的C3a受体拮抗剂SB290157。UUO模型小鼠和假手术小鼠每12小时皮下注射Cp40(1 mg/kg),每日腹腔注射SB290157(30 mg/kg)。7天或14天后,通过颈椎脱臼处死小鼠,并采集外周血、脾脏和肾脏组织。将小鼠肾脏用 4% 甲醛固定 24 小时,经梯度酒精脱水处理,并包埋于石蜡中。剩余的样本冷冻于液氮中以备后用。 |
| 毒性/毒理 (Toxicokinetics/TK) |
AMY-101局部注射剂量递增研究[1]
本研究旨在确定在患有自然发生的牙周炎的非人灵长类动物(NHP)中,局部注射递增浓度的AMY-101后是否会引起局部牙龈刺激。测试的AMY-101剂量递增分别为2、10、50、100和200 mg/mL,总体积为50 μL,分别对应于每个注射部位0.1、0.5、2.5、5和10 mg。注射部位包括上颌(腭侧牙间乳头)和下颌(颊侧牙间乳头)两侧的后牙。本研究使用了5只动物,所有注射均在一次给药过程中完成,随后进行为期2周的观察。每天检查动物是否存在因AMY-101注射引起的局部牙龈刺激。浓度等于或高于 10 mg/mL 的药物会引起轻度至中度炎症,且在最高剂量(100 和 200 mg/mL)下更为常见(图 2)。在所有治疗部位,2 mg/mL 剂量均未观察到刺激反应,这与上述数据一致。在基线以及治疗后 1 周和 2 周进行临床检查以确定牙周疾病活动度并拍摄口内照片。在疗效方面,浓度高达 50 mg/mL 的药物可降低牙周临床参数(探诊深度 [PPD]、临床附着水平 [CAL] 和牙龈指数 [GI])(图 3)。相反,最高剂量(100 和 200 mg/mL)则导致上述临床参数恶化(图 3)。因此,在所测试的不同 AMY-101 浓度中,2 mg/mL 的剂量似乎是满足安全性和保护性要求的最佳剂量。 |
| 参考文献 |
|
| 其他信息 |
AMY-101,又名补体抑制剂40(compstatin 40),是一种肽类补体核心成分C3抑制剂。AMY-101目前正在临床试验NCT03694444(一项关于C3补体抑制剂AMY-101治疗成人牙龈炎的研究)中进行研究。
C3补体抑制剂AMY-101是一种基于补体抑制剂的C3抑制剂,可抑制人补体成分C3,具有治疗多种以补体过度激活为关键因素的疾病的潜力,包括阵发性睡眠性血红蛋白尿症(PNH)和补体3肾小球病(C3G)。给药后,C3补体抑制剂AMY-101选择性地与C3结合并抑制C3活性。这可以阻止补体途径的激活,并抑制补体介导的炎症和细胞溶解。补体过度激活在多种炎症性和自身免疫性疾病中起着关键作用,并会导致组织破坏。 C3是补体系统的关键核心成分,而补体系统又是先天免疫反应的重要组成部分。 牙周炎是一种与补体系统过度激活相关的慢性炎症性疾病。近期临床前研究表明,宿主调节疗法可能有助于有效治疗人类牙周炎,若不及时治疗,牙周炎可能导致牙齿脱落和功能丧失。我们此前已证实,局部给药的AMY-101(Cp40,一种补体核心成分C3的肽类抑制剂)每周一次,即可抑制非人灵长类动物(NHP)自然发生的牙周炎。本研究旨在确定增加药物剂量后的局部安全性,以及降低给药频率或在全身给药后使用该药物的疗效。我们的研究结果确定了AMY-101的局部给药剂量(0.1 mg/位点),该剂量每3周给药一次,既不会引起局部刺激,又能有效治疗牙周炎。此外,每日皮下注射AMY-101(4 mg/kg体重)可预防非人灵长类动物牙周炎,提示接受全身性疾病(例如阵发性睡眠性血红蛋白尿)治疗的患者,其牙周状况也可能得到改善。总之,AMY-101似乎是一种有前景的人类牙周炎辅助治疗候选药物,这一观点值得在人体临床试验中进行验证。[1] 急性呼吸窘迫综合征(ARDS)是COVID-19肺炎的一种严重临床表现,主要由免疫驱动的病理机制引起。越来越多的证据表明,COVID-19是由宿主适应不良的炎症反应所驱动,这种反应涉及先天免疫通路的过度激活。虽然已证实存在涉及IL-6和其他细胞因子的“细胞因子风暴”,但补体C3激活被认为是SARS-CoV感染临床前模型中加剧肺损伤的初始效应机制。靶向C3的干预措施可能为COVID-19患者提供更广泛的补体介导的炎症损伤治疗控制。本文报道了一例因COVID-19肺炎导致严重ARDS的患者,该患者安全有效地接受了基于补体抑制剂的C3抑制剂AMY-101治疗。[2] 补体合成在来源细胞中与肾脏疾病的发病机制和进展密切相关。多项研究已探讨了肾脏疾病中的局部C3合成,并阐明了局部细胞来源的作用,但浸润性炎症细胞的作用仍不清楚。我们研究了C3、巨噬细胞和Th17细胞之间的关系,这些细胞均参与间质纤维化。本文报道,在肾活检标本中检测到局部C3表达增加,主要由单核细胞/巨噬细胞介导,且与肾纤维化(RF)的严重程度和肾功能指标相关。在单侧输尿管梗阻(UUO)小鼠模型中,我们发现局部C3在肾脏间质中组成性表达,并由F4/80+巨噬细胞释放。使用氯膦酸盐清除巨噬细胞后,缺乏巨噬细胞的小鼠表现出C3表达和肾小管间质纤维化的减少。使用C3和C3aR抑制剂阻断C3表达可对肾小管间质纤维化提供类似的保护作用。这些保护作用与促炎细胞因子减少、炎症细胞肾脏募集减少以及Th17反应减弱有关。体外实验表明,重组C3a显著增强T细胞增殖和IL-17A表达,其机制是通过T细胞中ERK、STAT3和STAT5的磷酸化以及NF-κB的激活。更重要的是,使用C3aR抑制剂阻断C3a可显著抑制C3a刺激的T细胞中IL-17A的表达。我们推测,巨噬细胞局部分泌C3可导致IL-17A介导的炎症细胞浸润肾脏,进而促进纤维化反应。我们的研究结果提示,抑制C3a/C3aR通路是治疗梗阻性肾病的一种新型治疗方法。[3] |
| 分子式 |
C83H117N23O18S2
|
|---|---|
| 分子量 |
1789.09039473534
|
| 精确质量 |
1787.838
|
| 元素分析 |
C, 55.72; H, 6.59; N, 18.01; O, 16.10; S, 3.58
|
| CAS号 |
1427001-89-5
|
| 相关CAS号 |
AMY-101 TFA;1789738-04-0;AMY-101 acetate
|
| PubChem CID |
131634231
|
| 序列 |
{D-Tyr}-Ile-Cys-Val-{Trp(Me)}-Gln-Asp-Trp-{Sar}-Ala-His-Arg-Cys-{N(Me)Ile}-NH2 (Disulfide bridge:Cys3-Cys13); H-D-Tyr-Ile-Cys(1)-Val-Trp(Me)-Gln-Asp-Trp-Sar-Ala-His-Arg-Cys(1)-N(Me)Ile-NH2;
D-tyrosyl-L-isoleucyl-L-cysteinyl-L-valyl-N1-methyl-L-tryptophyl-L-glutaminyl-L-alpha-aspartyl-L-tryptophyl-sarcosyl-L-alanyl-L-histidyl-L-arginyl-L-cysteinyl-N2-methyl-L-isoleucinamide (3->13)-disulfide
|
| 短序列 |
YICVXQDWGAHRCI; {D-Tyr}-ICV-{Trp(Me)}-QDW-{Sar}-AHRC-{N(Me)Ile}-NH2 (Disulfide bridge:Cys3-Cys13)
|
| 外观&性状 |
White to off-white solid powder
|
| LogP |
-2.1
|
| tPSA |
692
|
| 氢键供体(HBD)数目 |
21
|
| 氢键受体(HBA)数目 |
23
|
| 可旋转键数目(RBC) |
30
|
| 重原子数目 |
126
|
| 分子复杂度/Complexity |
3770
|
| 定义原子立体中心数目 |
15
|
| SMILES |
CC[C@H](C)[C@@H](C(=O)N[C@H]1CSSC[C@H](NC(=O)[C@@H](NC(=O)[C@@H](NC(=O)[C@@H](NC(=O)CN(C(=O)[C@@H](NC(=O)[C@@H](NC(=O)[C@@H](NC(=O)[C@@H](NC(=O)[C@@H](NC1=O)C(C)C)CC2=CN(C3=CC=CC=C32)C)CCC(=O)N)CC(=O)O)CC4=CNC5=CC=CC=C54)C)C)CC6=CN=CN6)CCCNC(=N)N)C(=O)N(C)[C@@H]([C@@H](C)CC)C(=O)N)NC(=O)[C@@H](CC7=CC=C(C=C7)O)N
|
| InChi Key |
MUSGYEMSJUFFHT-UWABRSFTSA-N
|
| InChi Code |
InChI=1S/C83H117N23O18S2/c1-11-43(5)68(103-72(114)53(84)30-46-23-25-50(107)26-24-46)80(122)100-61-39-125-126-40-62(82(124)106(10)69(70(86)112)44(6)12-2)101-73(115)55(21-17-29-90-83(87)88)94-76(118)58(33-49-36-89-41-92-49)96-71(113)45(7)93-65(109)38-105(9)81(123)60(31-47-35-91-54-20-15-13-18-51(47)54)99-77(119)59(34-66(110)111)97-74(116)56(27-28-64(85)108)95-75(117)57(98-79(121)67(42(3)4)102-78(61)120)32-48-37-104(8)63-22-16-14-19-52(48)63/h13-16,18-20,22-26,35-37,41-45,53,55-62,67-69,91,107H,11-12,17,21,27-34,38-40,84H2,1-10H3,(H2,85,108)(H2,86,112)(H,89,92)(H,93,109)(H,94,118)(H,95,117)(H,96,113)(H,97,116)(H,98,121)(H,99,119)(H,100,122)(H,101,115)(H,102,120)(H,103,114)(H,110,111)(H4,87,88,90)/t43-,44-,45-,53+,55-,56-,57-,58-,59-,60-,61-,62-,67-,68-,69-/m0/s1
|
| 化学名 |
2-((4R,7S,10S,13S,19S,22S,25S,28S,31S,34R)-10-((1H-imidazol-5-yl)methyl)-19-((1H-indol-3-yl)methyl)-34-((2S,3S)-2-((R)-2-amino-3-(4-hydroxyphenyl)propanamido)-3-methylpentanamido)-4-(((2S,3S)-1-amino-3-methyl-1-oxopentan-2-yl)(methyl)carbamoyl)-25-(3-amino-3-oxopropyl)-7-(3-guanidinopropyl)-31-isopropyl-13,17-dimethyl-28-((1-methyl-1H-indol-3-yl)methyl)-6,9,12,15,18,21,24,27,30,33-decaoxo-1,2-dithia-5,8,11,14,17,20,23,26,29,32-decaazacyclopentatriacontan-22-yl)acetic acid
|
| 别名 |
AMY-101; AMY 101; AMY101; Compstatin 40; 1427001-89-5; UNII-4Z4DFR9BX7; 4Z4DFR9BX7; peptide 14 [PMID: 22795972]; S3,S13-Cyclo(D-tyrolsyl-L-isoleucyl-L-cysteinyl-L-valyl-1-methyl-L-tryptophyl-L-glutaminyl-L-aspartyl-L-tryptophyl-N-methyl-L-glycyl-L-alanyl-L-histidyl-L-arginyl-L-cysteinyl-N-methyl-L-isoleucinamide); Compstatin 40; CP40; CP 40; CP-40;
|
| HS Tariff Code |
2934.99.9001
|
| 存储方式 |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| 运输条件 |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| 溶解度 (体外实验) |
May dissolve in DMSO (in most cases), if not, try other solvents such as H2O, Ethanol, or DMF with a minute amount of products to avoid loss of samples
|
|---|---|
| 溶解度 (体内实验) |
注意: 如下所列的是一些常用的体内动物实验溶解配方,主要用于溶解难溶或不溶于水的产品(水溶度<1 mg/mL)。 建议您先取少量样品进行尝试,如该配方可行,再根据实验需求增加样品量。
注射用配方
注射用配方1: DMSO : Tween 80: Saline = 10 : 5 : 85 (如: 100 μL DMSO → 50 μL Tween 80 → 850 μL Saline)(IP/IV/IM/SC等) *生理盐水/Saline的制备:将0.9g氯化钠/NaCl溶解在100 mL ddH ₂ O中,得到澄清溶液。 注射用配方 2: DMSO : PEG300 :Tween 80 : Saline = 10 : 40 : 5 : 45 (如: 100 μL DMSO → 400 μL PEG300 → 50 μL Tween 80 → 450 μL Saline) 注射用配方 3: DMSO : Corn oil = 10 : 90 (如: 100 μL DMSO → 900 μL Corn oil) 示例: 以注射用配方 3 (DMSO : Corn oil = 10 : 90) 为例说明, 如果要配制 1 mL 2.5 mg/mL的工作液, 您可以取 100 μL 25 mg/mL 澄清的 DMSO 储备液,加到 900 μL Corn oil/玉米油中, 混合均匀。 View More
注射用配方 4: DMSO : 20% SBE-β-CD in Saline = 10 : 90 [如:100 μL DMSO → 900 μL (20% SBE-β-CD in Saline)] 口服配方
口服配方 1: 悬浮于0.5% CMC Na (羧甲基纤维素钠) 口服配方 2: 悬浮于0.5% Carboxymethyl cellulose (羧甲基纤维素) 示例: 以口服配方 1 (悬浮于 0.5% CMC Na)为例说明, 如果要配制 100 mL 2.5 mg/mL 的工作液, 您可以先取0.5g CMC Na并将其溶解于100mL ddH2O中,得到0.5%CMC-Na澄清溶液;然后将250 mg待测化合物加到100 mL前述 0.5%CMC Na溶液中,得到悬浮液。 View More
口服配方 3: 溶解于 PEG400 (聚乙二醇400) 请根据您的实验动物和给药方式选择适当的溶解配方/方案: 1、请先配制澄清的储备液(如:用DMSO配置50 或 100 mg/mL母液(储备液)); 2、取适量母液,按从左到右的顺序依次添加助溶剂,澄清后再加入下一助溶剂。以 下列配方为例说明 (注意此配方只用于说明,并不一定代表此产品 的实际溶解配方): 10% DMSO → 40% PEG300 → 5% Tween-80 → 45% ddH2O (或 saline); 假设最终工作液的体积为 1 mL, 浓度为5 mg/mL: 取 100 μL 50 mg/mL 的澄清 DMSO 储备液加到 400 μL PEG300 中,混合均匀/澄清;向上述体系中加入50 μL Tween-80,混合均匀/澄清;然后继续加入450 μL ddH2O (或 saline)定容至 1 mL; 3、溶剂前显示的百分比是指该溶剂在最终溶液/工作液中的体积所占比例; 4、 如产品在配制过程中出现沉淀/析出,可通过加热(≤50℃)或超声的方式助溶; 5、为保证最佳实验结果,工作液请现配现用! 6、如不确定怎么将母液配置成体内动物实验的工作液,请查看说明书或联系我们; 7、 以上所有助溶剂都可在 Invivochem.cn网站购买。 |
| 制备储备液 | 1 mg | 5 mg | 10 mg | |
| 1 mM | 0.5589 mL | 2.7947 mL | 5.5894 mL | |
| 5 mM | 0.1118 mL | 0.5589 mL | 1.1179 mL | |
| 10 mM | 0.0559 mL | 0.2795 mL | 0.5589 mL |
1、根据实验需要选择合适的溶剂配制储备液 (母液):对于大多数产品,InvivoChem推荐用DMSO配置母液 (比如:5、10、20mM或者10、20、50 mg/mL浓度),个别水溶性高的产品可直接溶于水。产品在DMSO 、水或其他溶剂中的具体溶解度详见上”溶解度 (体外)”部分;
2、如果您找不到您想要的溶解度信息,或者很难将产品溶解在溶液中,请联系我们;
3、建议使用下列计算器进行相关计算(摩尔浓度计算器、稀释计算器、分子量计算器、重组计算器等);
4、母液配好之后,将其分装到常规用量,并储存在-20°C或-80°C,尽量减少反复冻融循环。
计算结果:
工作液浓度: mg/mL;
DMSO母液配制方法: mg 药物溶于 μL DMSO溶液(母液浓度 mg/mL)。如该浓度超过该批次药物DMSO溶解度,请首先与我们联系。
体内配方配制方法:取 μL DMSO母液,加入 μL PEG300,混匀澄清后加入μL Tween 80,混匀澄清后加入 μL ddH2O,混匀澄清。
(1) 请确保溶液澄清之后,再加入下一种溶剂 (助溶剂) 。可利用涡旋、超声或水浴加热等方法助溶;
(2) 一定要按顺序加入溶剂 (助溶剂) 。
InvivoChem的所有产品仅用于作科学研究,不面向患者销售
Copyright 2020 InvivoChem LLC | All Rights Reserved 粤ICP备20063088号-1
































 COA
COA
 463611831
463611831
