| 规格 | 价格 | 库存 | 数量 |
|---|---|---|---|
| 1mg |
|
||
| 5mg |
|
||
| 10mg |
|
||
| Other Sizes |
|

| 靶点 |
GIP (glucose-dependent insulin nutritive polypeptide); GLP-1 (glucagon-like peptide-1) receptor
Tirzepatide is a dual agonist that targets two distinct G protein-coupled receptors: the glucose-dependent insulinotropic polypeptide (GIP) receptor and the glucagon-like peptide-1 (GLP-1) receptor [39L4-L5]. These receptors are key incretin hormones that are naturally released in response to food intake. By activating both receptors simultaneously, tirzepatide produces a synergistic effect on insulin secretion (only when glucose is elevated), suppresses glucagon secretion, delays gastric emptying, and reduces appetite centrally, leading to improved glycemic control and significant weight loss. Tirzepatide shows biased signaling at the GLP-1 receptor and differentially induces internalization of the GIPR versus the GLP-1R. |
|---|---|
| 体外研究 (In Vitro) |
替泽帕肽(LY3298176)在减重和血糖控制方面显示出比度拉糖肽显著更高的疗效[1]。替泽帕肽是GIPR和GLP-1R的失衡激动剂,并在GLP-1R处表现出偏向性信号传导。替泽帕肽对GIPR和GLP-1R的内化作用存在差异[2]。
体外研究证实,替泽帕肽是一种高效的双重激动剂。与选择性GLP-1受体激动剂度拉糖肽(一种糖尿病标准治疗药物)相比,替泽帕肽在减重和血糖控制方面均表现出显著更高的疗效。其体外活性特征在于激活GIP和GLP-1受体,从而导致表达这些受体的细胞系中环磷酸腺苷(cAMP)积累增加。这种偏向性信号传导模式是其独特疗效的关键所在。 |
| 体内研究 (In Vivo) |
在控制血糖和促进减肥方面,盐酸特泽帕肽(LY3298176 盐酸盐)明显比度拉鲁肽更有效[1]。
体内实验表明,盐酸替泽帕肽是一种高效的治疗药物。临床试验显示,其在控制血糖和促进体重减轻方面显著优于度拉糖肽和其他对照药物。盐酸替泽帕肽可同时激活GIP和GLP-1受体,从而显著且持续地降低HbA1c(长期血糖指标)水平,并显著减轻2型糖尿病和/或肥胖患者的体重,其疗效优于选择性GLP-1受体激动剂。 |
| 酶活实验 |
与人GLP-1(7-36)NH2、GIP(1-42)、替拉帕肽和索玛鲁肽的竞争性结合实验基本按照同源竞争实验所述方法进行,不同之处在于测定缓冲液为1.0 mM MgCl2、2.5 mM CaCl2、0.003% (w/v) Tween-20和0.1% (w/v)杆菌肽,溶于25 mM HEPES缓冲液(pH 7.4),最终浓度为[125I]GLP-1(7-36)NH2或[125I]GIP(1-42)与GLP-1R和GIPR膜结合的Bmax值,以结合量与所添加的竞争性同源肽浓度的关系进行非线性回归分析。Bmax值用于计算每个细胞的受体数量。对于竞争性肽,采用非线性回归分析,以[125I]GLP-1(7-36)NH2或[125I]GIP(1-42)结合量与添加肽的浓度为因变量,确定Ki值。[2]
替泽帕肽与GIP和GLP-1受体的结合可在无细胞实验中进行研究。GIP或GLP-1受体结合的标准方案是竞争性放射性配体结合实验,该实验使用表达人重组GIPR或GLP-1R的细胞膜。将细胞膜与固定浓度的放射性标记标准品(例如[125I]-GIP或[125I]-GLP-1)在递增浓度的替泽帕肽存在下孵育。孵育后,将混合物通过GF/B滤板过滤,并使用闪烁计数器测量结合的放射性。测定置换50%放射性配体所需的替泽帕肽浓度(IC50),即可获得其对每种受体的结合亲和力。 |
| 细胞实验 |
将稳定表达HA-GIPR-EFGP或HA-GLP-1R-EFGP克隆的HEK293细胞接种于聚赖氨酸包被的96孔微孔板中,培养至细胞汇合度达到80%–90%。在实验当天,移除培养基,用预热的饥饿培养基(不含血清和抗生素的培养基,添加0.1%酪蛋白)洗涤细胞一次,然后在37℃、5% CO2条件下用新鲜培养基平衡1小时。在预热的饥饿培养基中制备GLP-1、GIP和替拉肽的浓度-反应曲线,将药物加入细胞中,并在指定时间点孵育,于37℃孵育。实验结束后,移除培养基,将细胞置于冰上,并用Prefer固定液(Anatech)固定10分钟。去除固定剂后,用PBS洗涤细胞,并用Odyssey封闭缓冲液(Licor)封闭1小时。将细胞与抗HA/DyLight800抗体(1:700)(Rockland Immunochemicals,600-445-384)孵育1小时,然后用PBS-T洗涤。使用配备800 nm激光通道的Licor Clx扫描仪扫描每个孔,以捕获荧光信号。数据以GLP-1或GIP的最大浓度(100%)和无配体(0%)进行标准化,并使用非线性回归(S型浓度-反应曲线)进行分析,最后使用GraphPad Prism 7软件作图。[2]
体外功能活性可通过基于细胞的 cAMP 积累测定法进行评估。将经基因工程改造可稳定表达人 GIP 或 GLP-1 受体的细胞(例如 CHO 或 HEK-293 细胞)接种于 96 孔板中。然后在 37℃ 下用不同浓度的替唑帕肽处理 30 分钟。使用均相时间分辨荧光 (HTRF) 或基于发光的检测试剂盒(例如 Cisbio cAMP 试剂盒或 PerkinElmer AlphaScreen)测量细胞内产生的 cAMP 量。受体激活的半数有效浓度 (EC50) 由剂量反应曲线计算得出。 |
| 动物实验 |
高脂饮食和链脲佐菌素注射诱导的糖尿病大鼠每周腹腔注射一次替拉帕肽(1.35 mg/kg)。采用莫里斯水迷宫实验、免疫荧光和蛋白质印迹分析评估其保护作用。采用高尔基染色法定量树突棘。[4]
雄性Sprague Dawley大鼠,体重180~200 g(7~8周龄),饲养于SPF级(无特定病原体)条件下,光照/黑暗周期为12 h/12 h,温度和湿度控制在22°C ± 1°C,50% ± 10%。所有实验程序均经湖北科技学院动物伦理委员会批准(IACUC编号:2021-03-003)。动物的饲养和处理均按照《实验动物管理声明》进行。经过两周的正常饮食适应后,共32只大鼠饲喂高脂饮食(67.5%标准实验室大鼠饲料,20%糖,10%猪油,2%胆固醇和0.5%胆盐),另有24只大鼠饲喂标准饲料。根据我们之前的研究,高脂饮食组大鼠腹腔注射35 mg/kg链脲佐菌素(STZ),而正常组大鼠仅注射柠檬酸盐缓冲液。两周后,将31只空腹血糖水平达到11.0 mmol/L的大鼠随机分为两组:糖尿病组(DM)和DM+替唑帕肽组(替唑帕肽,1.35 mg/kg,每周一次)。同时,将24只标准饲料组的大鼠随机分为对照组(Con)和Con+替拉西肽组(替拉西肽,1.35 mg/kg,每周一次)。所有药物均在特定条件下制备,可保存1年以上,避免降解。于第13周进行口服葡萄糖耐量试验(OGTT)。在处死前进行行为学测试。每周测量空腹血糖和体重,直至处死。第15周,处死所有大鼠并采集样本,用于后续实验。实验流程图见图1A。[4] 替尔泽帕肽的体内动物研究通常在糖尿病和肥胖的啮齿动物模型中进行。雄性C57BL/6J小鼠喂食高脂饮食以诱导肥胖,每日皮下注射替尔泽帕肽盐酸盐,剂量范围为0.1至10 mg/kg。每日测量体重和食物摄入量。为评估血糖控制情况,进行腹腔葡萄糖耐量试验(IPGTT):小鼠禁食过夜后,腹腔注射葡萄糖(例如,2 g/kg),并在0、15、30、60和120分钟时使用血糖仪测量血糖水平。计算药物对血糖波动和曲线下面积(AUC)的影响。 |
| 药代性质 (ADME/PK) |
吸收、分布和排泄
在1-5 mg的剂量范围内,替扎帕特的Cmax为108-397 ng/mL。皮下注射后替扎帕特的平均绝对生物利用度为80%。皮下注射后的Tmax为8-72小时。每周皮下注射4周后可达到稳态血浆浓度。由于替扎帕特会延缓胃排空,因此可能会影响同时服用的口服药物的吸收。美国处方信息建议,当替扎帕特与其他口服药物同时使用时应谨慎。替扎帕特主要经尿液和粪便排泄,大部分以代谢物的形式排出。在尿液或粪便中未检测到代谢产物。皮下注射后平均稳态分布容积为 9.5 L。在 2 型糖尿病患者中,皮下注射替唑帕特后平均表观稳态分布容积约为 10.3 L。 替唑帕林的表观群体清除率为 0.061 L/h。替唑帕林的平均稳态表观清除率为 0.056 L/h。 代谢/代谢物 替唑帕林通过肽骨架的蛋白水解、C20 脂肪酸部分的 β-氧化和酰胺水解进行代谢。 生物半衰期 半衰期约为五天。 替泽帕肽配制成皮下注射液。其药代动力学特征为吸收缓慢、末端半衰期长(在人体内约为5天)和生物利用度高。较长的半衰期支持每周一次给药。较长的半衰期是通过在分子上添加一个C20脂肪酸二酸部分实现的,该部分与白蛋白结合,保护肽免受快速肾清除和蛋白水解降解。盐酸盐形式用于药物固体制剂中,以确保其在生产和储存过程中的稳定性。 |
| 毒性/毒理 (Toxicokinetics/TK) |
肝毒性
在注册前临床试验中,接受替扎帕肽治疗的患者中,血清转氨酶升高超过正常值上限 (ULN) 3 倍的发生率低于 1%,安慰剂组和对照组的发生率相似。在涉及 5000 多例患者的研究中,未报告替扎帕肽引起的严重肝功能障碍或具有临床意义的肝损伤。然而,替扎帕肽与急性胆囊疾病(胆结石、胆汁性胆管炎和胆囊切除术)的发生率略有升高相关,治疗组的发生率为 0.6%,安慰剂组为 0%。替扎帕肽产品说明书的警告部分提到了胆囊疾病。概率评分:E(不太可能引起具有临床意义的肝损伤)。妊娠和哺乳期影响 ◉ 哺乳期用药概述 目前尚无关于替唑帕肽在哺乳期临床应用的信息。由于替唑帕肽是一种分子量为 4814 Da 的大肽分子,其在母乳中的含量可能非常低,并且由于可能在婴儿的胃肠道中部分被破坏,因此不太可能被吸收。在获得更多数据之前,哺乳期妇女应谨慎使用替唑帕肽,尤其是在哺乳新生儿或早产儿时。 ◉ 对母乳喂养婴儿的影响 截至修订日期,未找到已发表的信息。 ◉ 对哺乳和母乳的影响 截至修订日期,未找到已发表的信息。 ◈ 什么是替唑帕肽? 替唑帕肽是一种用于改善 2 型糖尿病成人患者血糖控制的药物。它以注射剂形式给药。该注射剂以商品名 Mounjaro® 销售。替佐帕肽也用于注射治疗肥胖症。用于体重管理的替佐帕肽以商品名 Zepbound® 销售。不建议在怀孕期间减肥。如果您正在使用 Zepbound®,请在更改用药前咨询您的医疗保健提供者。您的医疗保健提供者可以与您讨论治疗您病情的益处以及在怀孕期间不治疗的风险。肥胖和高血糖会使妊娠更加困难,并增加流产、出生缺陷或其他妊娠并发症的风险。有关糖尿病(https://mothertobaby.org/fact-sheets/type-1-and-type-2-diabetes/)和肥胖症(https://mothertobaby.org/fact-sheets/obesity-pregnancy/)的信息可在 MotherToBaby 网站上找到。替佐帕肽的产品标签指出,使用该药物可能会改变口服避孕药(用于预防妊娠的药片)在体内的吸收方式。即使正确且持续地服用口服避孕药,这仍可能增加怀孕的风险。产品标签建议,服用口服避孕药的人在开始服药后的4周内以及每次增加剂量后的4周内,应改用非口服避孕药或加用屏障避孕法(例如避孕套)。如果您正在服用此药,请与您的医疗保健提供者讨论非口服避孕方法以及所有预防怀孕的方案。 ◈ 我正在服用替唑拉肽,但我想在怀孕前停药。这种药物会在我体内停留多久? 每个人代谢(分解)药物所需的时间都不同。对于健康成年人来说,替唑拉肽平均需要长达30天才能从体内完全清除。 ◈ 我正在服用替唑拉肽。这会让我更难怀孕吗?目前尚不清楚替唑普拉肽是否会降低受孕几率。◈服用替唑普拉肽会增加流产风险吗?◈流产很常见,任何妊娠都可能发生,原因有很多。目前尚无人体研究证实替唑普拉肽会增加流产风险。◈服用替唑普拉肽会增加胎儿出生缺陷的风险吗?◈每次妊娠都有3-5%的出生缺陷风险,称为背景风险。目前尚无研究证实替唑普拉肽会增加人类胎儿出生缺陷的风险。动物研究发现替唑普拉肽会增加某些出生缺陷的风险。然而,尚不清楚这些出生缺陷是由药物本身引起的,还是由研究中的其他因素(例如体重减轻)引起的。妊娠期糖尿病控制不佳可能会增加胎儿出生缺陷的风险。妊娠期糖尿病的控制至关重要,整个孕期血糖水平都应保持在目标范围内。 ◈ 妊娠期服用替唑拉肽会增加其他妊娠相关问题的风险吗? 目前尚无人体研究证实替唑拉肽会增加早产(妊娠37周前分娩)或低出生体重(出生体重低于5磅8盎司[2500克])等妊娠相关问题的风险。动物研究报告称,妊娠期接触替唑拉肽后,后代体重有所下降。目前尚不清楚这是由于药物本身、母体体重减轻还是其他因素所致。妊娠期糖尿病控制不佳会增加妊娠并发症的风险。 ◈ 妊娠期服用替唑拉肽会影响孩子未来的行为或学习能力吗? 目前尚无研究评估替唑拉肽是否会增加儿童出现行为或学习问题的风险。 ◈ 服用替佐帕肽期间哺乳: 目前尚无关于替佐帕肽与母乳之间关系的信息。由于替佐帕肽分子较大,预计不会大量进入母乳。此外,该药物可能在婴儿的胃肠道内分解,吸收不良。如有任何与母乳喂养相关的问题,请咨询您的医疗保健提供者。 ◈ 男性服用替佐帕肽是否会影响生育能力或增加出生缺陷的风险? 目前尚无人体研究确定替佐帕肽是否会影响男性生育能力(使伴侣怀孕的能力)或增加出生缺陷的风险(高于背景风险)。一项动物研究报告称,男性生育能力未发生变化。通常情况下,与孩子父亲或精子捐赠者接触不太可能增加怀孕的风险。更多信息,请参阅 MotherToBaby 网站上的“父亲接触”信息表,网址为 https://mothertobaby.org/fact-sheets/paternal-exposures-pregnancy/。 蛋白质结合 替佐帕肽与血浆白蛋白的结合率达 99%。 替泽帕肽盐酸盐的毒性已在临床前(动物)和临床(人体)研究中得到广泛研究。替泽帕肽最常见的不良反应是胃肠道反应(恶心、腹泻、呕吐、便秘、腹痛),这些反应通常为轻度至中度,并会随时间推移而减轻。胰腺炎、胆囊疾病以及甲状腺C细胞肿瘤(包括甲状腺髓样癌)的风险等严重毒性反应是潜在风险,已在警告和注意事项中予以明确标注。对于有甲状腺髓样癌(MTC)个人史或家族史的患者,以及患有2型多发性内分泌肿瘤综合征(MEN 2)的患者,禁用替泽帕肽。 |
| 参考文献 |
[1]. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: a randomised, placebo-controlled and active comparator-controlled phase 2 trial. Lancet. 2018 Nov 17;392(10160):2180-2193.
[2]. Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight. 2020 Sep 3; 5(17): e140532. [3]. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Mol Metab. 2018 Dec:18:3-14. [4]. Tirzepatide ameliorates spatial learning and memory impairment through modulation of aberrant insulin resistance and inflammation response in diabetic rats. Front Pharmacol. 2023 Aug 28;14:1146960. |
| 其他信息 |
药效学
替拉肽是一种具有降血糖作用的合成肽。它通过刺激胰岛素分泌的第一时相和第二时相,并降低胰高血糖素水平,发挥其葡萄糖依赖性降血糖作用。研究表明,替拉肽还能延缓胃排空,降低空腹和餐后血糖浓度,减少食物摄入,并减轻2型糖尿病患者的体重。替拉肽可以改善胰岛素敏感性。由于该肽通过亲水连接子与第20位赖氨酸残基上的C20脂肪酸部分偶联,因此该药物在血浆中与白蛋白高度结合,从而延长了其半衰期。背景:LY3298176是一种新型的双重葡萄糖依赖性促胰岛素肽(GIP)和胰高血糖素样肽-1(GLP-1)受体激动剂,目前正在开发用于治疗2型糖尿病。本研究旨在探讨LY3298176在血糖控制不佳的2型糖尿病患者中的疗效和安全性,并与安慰剂或选择性GLP-1受体激动剂度拉糖肽进行比较。方法:在这项双盲、随机、II期研究中,2型糖尿病患者按1:1:1:1:1的比例随机分组,分别接受每周一次皮下注射LY3298176(1 mg、5 mg、10 mg或15 mg)、度拉糖肽(1.5 mg)或安慰剂,疗程为26周。分组依据基线糖化血红蛋白A1c(HbA1c)、二甲双胍使用情况和体重指数(BMI)进行分层。符合条件的受试者(年龄 18 至 75 岁),患有 2 型糖尿病至少 6 个月(糖化血红蛋白 HbA1c 为 7.0% 至 10.5%,含 7.0% 和 10.5%),仅通过饮食和运动或稳定的二甲双胍治疗无法充分控制血糖,且体重指数 (BMI) 为 23 至 50 kg/m²。主要疗效终点为改良意向性治疗 (mITT) 人群(所有接受过至少一次研究药物治疗且至少有一次基线后任何结局指标测量值的患者)中 HbA1c 从基线到第 26 周的变化。次要终点在 mITT 治疗数据集中测量,包括 HbA1c 从基线到第 12 周的变化;平均体重、空腹血糖、腰围、总胆固醇、低密度脂蛋白胆固醇、高密度脂蛋白胆固醇和甘油三酯的变化;本研究评估了从基线到第12周和第26周达到HbA1c目标值(≤6.5%和<7.0%)的患者比例的变化,以及从基线到第26周体重减轻至少5%和10%的患者比例。该研究已在ClinicalTrials.gov网站注册,注册号为NCT03131687。结果:2017年5月24日至2018年3月28日期间,共评估了555名受试者的入组资格,其中318名受试者被随机分配到六个治疗组之一。由于两名受试者未接受治疗,因此改良的意向性治疗分析和安全性分析人群共包含316名受试者。258名(81.7%)受试者完成了26周的治疗,283名(89.6%)受试者完成了研究。基线时,平均年龄为 57 岁(标准差 9),BMI 为 32.6 kg/m²(5.9),糖尿病确诊病程为 9 年(6),HbA1c 为 8.1%(1.0),53% 的患者为男性,47% 为女性。第 26 周时,LY3298176 对 HbA1c 变化的影响呈剂量依赖性,且未达到平台期。与安慰剂相比,LY3298176 治疗后 HbA1c 较基线的平均变化分别为:1 mg 组 -1.06%,5 mg 组 -1.73%,10 mg 组 -1.89%,15 mg 组 -1.94%(安慰剂组为 -0.06%)(与安慰剂相比,后验平均差异 [80% 置信区间]:1 mg 组 -1.00% [-1.22 至 -0.79],5 mg 组 -1.67% [-1.88 至 -1.46],10 mg 组 -1.83% [-2.04 至 -1.61],15 mg 组 -1.89% [-2.11 至 -1.67])。与度拉糖肽(-1.21%)相比,LY3298176 剂量组从基线到 26 周 HbA1c 变化的后验平均差异(80% 置信区间)分别为:1 mg 剂量组 0.15%(-0.08 至 0.38),5 mg 剂量组 -0.52%(-0.72 至 -0.31),10 mg 剂量组 -0.67%(-0.89 至 -0.46),15 mg 剂量组 -0.73%(-0.95 至 -0.52)。在第26周,接受LY3298176治疗的患者中,33%至90%达到HbA1c低于7.0%的目标水平(度拉糖肽组为52%,安慰剂组为12%),15%至82%达到HbA1c至少6.5%的目标水平(度拉糖肽组为39%,安慰剂组为2%)。LY3298176组的空腹血糖水平范围为-0.4 mmol/L至-3.4 mmol/L(安慰剂组为0.9 mmol/L,度拉糖肽组为-1.2 mmol/L)。LY3298176组的平均体重减轻范围为-0.9 kg至-11.3 kg(安慰剂组为0.4 kg,度拉糖肽组为-2.7 kg)。在第26周,接受LY3298176治疗的患者中,14%至71%达到了至少5%的减重目标(度拉糖肽组为22%,安慰剂组为0%),6%至39%达到了至少10%的减重目标(度拉糖肽组为9%,安慰剂组为0%)。LY3298176组的腰围变化范围为-2.1厘米至-10.2厘米(安慰剂组为-1.3厘米,度拉糖肽组为-2.5厘米)。LY3298176组的总胆固醇变化范围为0.2毫摩尔/升至-0.3毫摩尔/升(安慰剂组为0.3毫摩尔/升,度拉糖肽组为-0.2毫摩尔/升)。 LY3298176组和安慰剂组的HDL或LDL胆固醇变化无显著差异。LY3298176组的甘油三酯浓度范围为0 mmol/L至-0.8 mmol/L(安慰剂组为0.3 mmol/L,度拉糖肽组为-0.3 mmol/L)。所有次要终点的12周和26周结果相似。在六个治疗组的316名受试者中,13名(4%)发生了23例严重不良事件。胃肠道事件(恶心、腹泻和呕吐)是治疗期间最常见的不良事件。胃肠道不良事件的发生率与剂量相关(1 mg LY3298176 组为 23.1%,5 mg LY3298176 组为 32.7%,10 mg LY3298176 组为 51.0%,15 mg LY3298176 组为 66.0%,度拉糖肽组为 42.6%,安慰剂组为 9.8%);大多数不良事件为轻度至中度且短暂。食欲下降是第二常见的不良事件(1 mg LY3298176 组为 3.8%,5 mg LY3298176 组为 20.0%,10 mg LY3298176 组为 25.5%,15 mg LY3298176 组为 18.9%,度拉糖肽组为 5.6%,安慰剂组为 2.0%)。未报告严重低血糖事件。安慰剂组有 1 例患者死于 IV 期肺腺癌,与研究治疗无关。结论:双重 GIP 和 GLP-1 受体激动剂 LY3298176 在血糖控制和体重减轻方面显示出比度拉糖肽更显著的疗效,且安全性和耐受性良好。GIP 和 GLP-1 受体的联合刺激可能为 2 型糖尿病提供一种新的治疗选择。 [1] 特拉泽肽 (LY3298176) 是一种双重 GIP 和 GLP-1 受体激动剂,目前正在开发用于治疗 2 型糖尿病 (T2DM)、肥胖症和非酒精性脂肪性肝炎。早期 T2DM 临床试验表明,特拉泽肽在改善临床疗效方面优于选择性 GLP-1 受体激动剂。因此,我们假设特拉泽肽的综合效力和信号转导特性赋予其独特的药理学特征,能够有效改善多种代谢控制。本文建立了一种计算该药物在临床有效剂量下各受体占有率的方法。分析结果表明,特拉泽肽与 GIP 受体的结合力强于与 GLP-1 受体的结合力,证实了其作用机制的不平衡性。药理学信号转导研究表明,替泽帕肽模拟天然GIP对GIP受体的作用,但对GLP-1受体表现出偏向性,倾向于促进cAMP生成而非β-arrestin募集,且其驱动GLP-1受体内化的能力也弱于GLP-1。原代胰岛实验表明,β-arrestin1限制了GLP-1而非GIP或替泽帕肽的胰岛素反应,提示替泽帕肽的偏向性激动剂效应增强了胰岛素分泌。GIP受体失衡以及GLP-1受体独特的信号转导特性可能共同解释了该研究药物的良好疗效。[2] 目的:开发一种新型的GIP和GLP-1双重受体激动剂LY3298176,以确定GIP的代谢效应是否能增强选择性GLP-1受体激动剂在2型糖尿病(T2DM)中已确立的临床获益。方法:LY3298176 是一种脂肪酸修饰肽,具有 GIP 和 GLP-1 受体双重激动剂活性,设计用于每周一次皮下注射。体外实验中,利用表达重组或内源性肠促胰岛素受体的细胞系对 LY3298176 进行信号转导和功能分析。体内实验中,通过小鼠体重、食物摄入量、胰岛素分泌和血糖谱对 LY3298176 进行表征。一项 I 期随机、安慰剂对照、双盲研究分为三个部分:首先,在健康受试者 (HS) 中进行单剂量递增 (SAD;剂量 0.25–8 mg) 研究和为期 4 周的多剂量递增 (MAD;剂量 0.5–10 mg) 研究;随后开展了一项为期 4 周的 Ib 期多剂量概念验证 (POC) 研究(剂量 0.5–15 mg),受试者为 2 型糖尿病 (T2DM) 患者(ClinicalTrials.gov 注册号:NCT02759107)。高于 5 mg 的剂量通过滴定获得,并以度拉糖肽 (DU) 作为阳性对照。本研究的主要目的是评估 LY3298176 的安全性和耐受性。结果:LY3298176 在体外激活了 GIP 和 GLP-1 受体信号通路,并在小鼠体内通过作用于 GIP 和 GLP-1 受体,表现出葡萄糖依赖性胰岛素分泌和改善葡萄糖耐量的作用。长期给予 LY3298176 可显著降低小鼠的体重和食物摄入量;这些作用显著强于 GLP-1 受体激动剂。共有142名受试者接受了至少一剂LY3298176、度拉糖肽或安慰剂。LY3298176的药代动力学研究在较宽的剂量范围(0.25–15 mg)内进行,结果支持每周一次的给药方案。在一项针对糖尿病患者的1b期试验中,与安慰剂相比,10 mg和15 mg剂量的LY3298176均显著降低了空腹血糖(最小二乘均值[LSM]差值[95% CI]分别为:-49.12 mg/dL [-78.14, -20.12]和-43.15 mg/dL [-73.06, -13.21])。在患有 MAD HS 的患者中,LY3298176 1.5 mg、4.5 mg 和 10 mg 剂量组的体重减轻幅度均显著大于安慰剂组(最小二乘均值差 [95% CI] 分别为:-1.75 kg [-3.38, -0.12]、-5.09 kg [-6.72, -3.46] 和 -4.61 kg [-6.21, -3.01])。10 mg 和 15 mg 剂量组在 2 型糖尿病患者中也显示出显著疗效(最小二乘均值差 [95% CI] 分别为:-2.62 kg [-3.79, -1.45] 和 -2.07 kg [-3.25, -0.88])。 LY3298176 最常见的不良反应是胃肠道反应(呕吐、恶心、食欲下降、腹泻和腹胀),这些反应在 HS 患者和 2 型糖尿病患者中均有发生。所有不良反应均呈剂量依赖性,且严重程度为轻度至中度。结论:基于这些结果,LY3298176 的药理学特性已从临床前研究转移到临床研究。LY3298176 有潜力在血糖控制和体重方面带来具有临床意义的改善。这些数据支持对 LY3298176 治疗 2 型糖尿病和潜在肥胖症进行进一步的临床评估。[3] 盐酸替西帕肽(LY3298176)是一种经美国食品药品监督管理局(FDA)批准上市的药物,用于治疗2型糖尿病(商品名:Mounjaro®)和作为饮食和运动辅助疗法用于慢性体重管理(商品名:Zepbound®)。它是由礼来公司研发的首创双重GIP/GLP-1受体激动剂。该药物的获批基于SURPASS(用于治疗糖尿病)和SURMOUNT(用于治疗肥胖症)两项3期临床试验项目的可靠临床数据,这些试验证实了其优于现有疗法。该药物适用于成人,且必须凭处方购买。它并非仅供研究使用,而是一种完全获批的药品。为了长期稳定性,通常以固体形式储存在4℃或-20℃的环境中。 |
| 分子式 |
C225H348N48O68.XHCL
|
|---|---|
| 相关CAS号 |
Tirzepatide;2023788-19-2;Tirzepatide TFA
|
| 序列 |
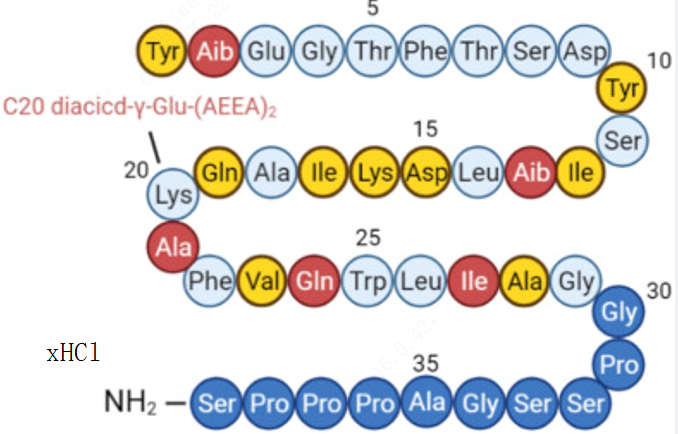
Tyr-{Aib}-Glu-Gly-Thr-Phe-Thr-Ser-Asp-Tyr-Ser-Ile-{Aib}-Leu-Asp-Lys-Ile-Ala-Gln-{C20 diacid-gamma-Glu-(AEEA)2-Lys}-Ala-Phe-Val-Gln-Trp-Leu-Ile-Ala-Gly-Gly-Pro-Ser-Ser-Gly-Ala-Pro-Pro-Pro-Ser-NH2
|
| 短序列 |
Y-{Aib}-EGTFTSDYSI-{Aib}-LDKIAQ-{C20 diacid-gamma-Glu-(AEEA)2-Lys}-AFVQWLIAGGPSSGAPPPS-NH2
|
| 外观&性状 |
White to off-white solid
|
| SMILES |
CC[C@H](C)[C@@H](C(=O)N[C@@H](C)C(=O)N[C@@H](CCC(=O)N)C(=O)N[C@@H](CCCCNC(=O)COCCOCCNC(=O)COCCOCCNC(=O)CC[C@H](C(=O)O)NC(=O)CCCCCCCCCCCCCCCCCCC(=O)O)C(=O)N[C@@H](C)C(=O)N[C@@H](CC1=CC=CC=C1)C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CCC(=O)N)C(=O)N[C@@H](CC2=CNC3=CC=CC=C32)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H](C)C(=O)NCC(=O)NCC(=O)N4CCC[C@H]4C(=O)N[C@@H](CO)C(=O)N[C@@H](CO)C(=O)NCC(=O)N[C@@H](C)C(=O)N5CCC[C@H]5C(=O)N6CCC[C@H]6C(=O)N7CCC[C@H]7C(=O)N[C@@H](CO)C(=O)N)NC(=O)[C@H](CCCCN)NC(=O)[C@H](CC(=O)O)NC(=O)[C@H](CC(C)C)NC(=O)C(C)(C)NC(=O)[C@H]([C@@H](C)CC)NC(=O)[C@H](CO)NC(=O)[C@H](CC8=CC=C(C=C8)O)NC(=O)[C@H](CC(=O)O)NC(=O)[C@H](CO)NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CC9=CC=CC=C9)NC(=O)[C@H]([C@@H](C)O)NC(=O)CNC(=O)[C@H](CCC(=O)O)NC(=O)C(C)(C)NC(=O)[C@H](CC1=CC=C(C=C1)O)N.CC(=O)O
|
| 别名 |
LY3298176; LY-3298176
|
| HS Tariff Code |
2934.99.9001
|
| 存储方式 |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month 注意: 请将本产品存放在密封且受保护的环境中,避免吸湿/受潮。 |
| 运输条件 |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| 溶解度 (体外实验) |
DMSO :~50 mg/mL
|
|---|---|
| 溶解度 (体内实验) |
Note: 如何溶解多肽产品?请参考本产品网页右上角“产品说明书“文件,第4页。 注意: 如下所列的是一些常用的体内动物实验溶解配方,主要用于溶解难溶或不溶于水的产品(水溶度<1 mg/mL)。 建议您先取少量样品进行尝试,如该配方可行,再根据实验需求增加样品量。 注射用配方
注射用配方1: DMSO : Tween 80: Saline = 10 : 5 : 85 (如: 100 μL DMSO → 50 μL Tween 80 → 850 μL Saline)(IP/IV/IM/SC等) *生理盐水/Saline的制备:将0.9g氯化钠/NaCl溶解在100 mL ddH ₂ O中,得到澄清溶液。 注射用配方 2: DMSO : PEG300 :Tween 80 : Saline = 10 : 40 : 5 : 45 (如: 100 μL DMSO → 400 μL PEG300 → 50 μL Tween 80 → 450 μL Saline) 注射用配方 3: DMSO : Corn oil = 10 : 90 (如: 100 μL DMSO → 900 μL Corn oil) 示例: 以注射用配方 3 (DMSO : Corn oil = 10 : 90) 为例说明, 如果要配制 1 mL 2.5 mg/mL的工作液, 您可以取 100 μL 25 mg/mL 澄清的 DMSO 储备液,加到 900 μL Corn oil/玉米油中, 混合均匀。 View More
注射用配方 4: DMSO : 20% SBE-β-CD in Saline = 10 : 90 [如:100 μL DMSO → 900 μL (20% SBE-β-CD in Saline)] 口服配方
口服配方 1: 悬浮于0.5% CMC Na (羧甲基纤维素钠) 口服配方 2: 悬浮于0.5% Carboxymethyl cellulose (羧甲基纤维素) 示例: 以口服配方 1 (悬浮于 0.5% CMC Na)为例说明, 如果要配制 100 mL 2.5 mg/mL 的工作液, 您可以先取0.5g CMC Na并将其溶解于100mL ddH2O中,得到0.5%CMC-Na澄清溶液;然后将250 mg待测化合物加到100 mL前述 0.5%CMC Na溶液中,得到悬浮液。 View More
口服配方 3: 溶解于 PEG400 (聚乙二醇400) 请根据您的实验动物和给药方式选择适当的溶解配方/方案: 1、请先配制澄清的储备液(如:用DMSO配置50 或 100 mg/mL母液(储备液)); 2、取适量母液,按从左到右的顺序依次添加助溶剂,澄清后再加入下一助溶剂。以 下列配方为例说明 (注意此配方只用于说明,并不一定代表此产品 的实际溶解配方): 10% DMSO → 40% PEG300 → 5% Tween-80 → 45% ddH2O (或 saline); 假设最终工作液的体积为 1 mL, 浓度为5 mg/mL: 取 100 μL 50 mg/mL 的澄清 DMSO 储备液加到 400 μL PEG300 中,混合均匀/澄清;向上述体系中加入50 μL Tween-80,混合均匀/澄清;然后继续加入450 μL ddH2O (或 saline)定容至 1 mL; 3、溶剂前显示的百分比是指该溶剂在最终溶液/工作液中的体积所占比例; 4、 如产品在配制过程中出现沉淀/析出,可通过加热(≤50℃)或超声的方式助溶; 5、为保证最佳实验结果,工作液请现配现用! 6、如不确定怎么将母液配置成体内动物实验的工作液,请查看说明书或联系我们; 7、 以上所有助溶剂都可在 Invivochem.cn网站购买。 |
计算结果:
工作液浓度: mg/mL;
DMSO母液配制方法: mg 药物溶于 μL DMSO溶液(母液浓度 mg/mL)。如该浓度超过该批次药物DMSO溶解度,请首先与我们联系。
体内配方配制方法:取 μL DMSO母液,加入 μL PEG300,混匀澄清后加入μL Tween 80,混匀澄清后加入 μL ddH2O,混匀澄清。
(1) 请确保溶液澄清之后,再加入下一种溶剂 (助溶剂) 。可利用涡旋、超声或水浴加热等方法助溶;
(2) 一定要按顺序加入溶剂 (助溶剂) 。
A Research Study to See How Much CagriSema (1.0 mg Once Weekly) Lowers Blood Sugar and Body Weight Compared to Tirzepatide (5 mg Once Weekly) in People With Type 2 Diabetes Treated With Metformin, SGLT2 Inhibitor or Both
CTID: NCT06534411
Phase: Phase 3 Status: R
A Randomized, Double-Blind, Placebo-Controlled Phase 2 Study Comparing
CTID: null
Phase: Phase 2 Status: Ongoing, GB - no longer in EU/EEA, Completed
Date: 2020-01-23
 TE-8105
TE-8105
 GEP44
GEP44
 Tifeglipron (CT-996)
Tifeglipron (CT-996)
 Naperiglipron
Naperiglipron
InvivoChem的所有产品仅用于作科学研究,不面向患者销售
Copyright 2020 InvivoChem LLC | All Rights Reserved 粤ICP备20063088号-1































 463611831
463611831
